In coronary intervention, seeing a narrowing on angiography does not automatically mean that the lesion is truly limiting blood flow. What matters clinically is whether that narrowing is already causing functional ischemia. That is why FFR pressure guidewires are important: they move decision-making from “how narrow does it look?” toward “how much is flow really affected?”
1. FFR matters because it answers whether a lesion is truly flow-limiting
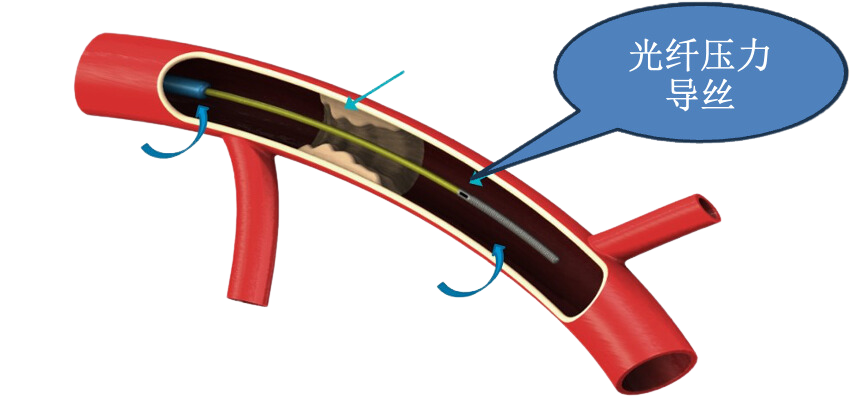
Fractional Flow Reserve (FFR) is a coronary physiology index. It does not simply describe anatomical narrowing. Instead, under maximal hyperemia, it uses a pressure guidewire to assess the pressure relationship across a lesion and determine whether that stenosis is functionally significant.
For clinical decisions, that matters because coronary treatment is not only about identifying a narrowing. It is about judging:
- whether the lesion is actually ischemia-producing
- whether revascularization is justified
- which lesion matters most when several are present
So the value of FFR is not just “measuring a number.” Its real importance is helping revascularization decisions rest on functional evidence.
2. Why FFR carries “gold-standard” meaning in functional assessment
In invasive coronary physiology, wire-based FFR has long been treated as a key reference standard. International guidelines continue to emphasize coronary physiology tools such as FFR and iFR because, in angiographically intermediate lesions or situations where the need for revascularization is uncertain, physiology-based assessment is more closely aligned with the real ischemic impact of the lesion than anatomy alone.
Public guidelines and reviews consistently support the idea that:
- coronary physiology has an important role in intermediate lesions
- FFR can guide revascularization decisions
- the field has shifted from angiography-only judgment toward combined anatomical and physiological assessment
That is why a website can describe an FFR pressure guidewire as:
“an important tool for coronary functional assessment and a key carrier of physiology-based decision-making.”
That framing is much stronger than simply saying the device “measures pressure.”
3. Why coronary angiography alone is not enough for functional blood-flow assessment
Coronary angiography remains fundamental, but it primarily answers an anatomical question: what does the vessel look like? Functional ischemia depends on more than percentage stenosis. It is influenced by:
- lesion length
- lesion geometry
- the amount of supplied myocardium
- serial lesion interaction
- collateral circulation
- microvascular status
That is why the literature repeatedly describes a visual-functional mismatch:
- a lesion that looks severe on angiography may not be functionally significant
- a lesion that looks only moderate may still produce important ischemia
In other words, angiography is indispensable for anatomy, but not always sufficient for judging whether blood flow is truly compromised. FFR remains important because it helps close the gap between appearance and physiological consequence.
4. The clinical value of an FFR pressure guidewire is not only diagnosis, but better decision support
From a website perspective, the strongest message is not merely that the guidewire can measure pressure. It is that it helps support better clinical decisions.
It helps identify lesions that really need treatment
In multivessel disease, serial disease, or intermediate stenosis, angiography alone may not define priority well. FFR helps focus intervention on lesions that are truly flow-limiting.
It may help avoid unnecessary stenting
If a lesion looks suspicious on angiography but is not functionally significant, the management pathway may differ from what anatomy alone would suggest.
It supports a more evidence-based revascularization strategy
Whether the choice is PCI, deferral, or further integrated assessment, physiology provides a stronger basis for that choice.
5. Why the fiber-optic pressure-sensing route deserves special attention
For your FFR program, the fiber-optic pressure sensor is not a secondary detail. It is one of the most meaningful technical differentiators.
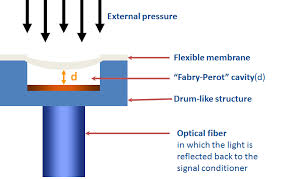
Public reviews describe several recurring advantages of optical-fiber pressure sensors in medical applications:
- strong miniaturization potential
- optical rather than conventional electrical signal transmission
- lower sensitivity to electromagnetic interference
- suitability for integration into guidewires, catheters, and other miniature devices
That matters especially in FFR, where the device sits at the intersection of miniaturization, structural precision, and sensitive physiologic measurement. On a website, the meaning of the fiber-optic route can be expressed on three levels:
- it is the sensing route used for pressure measurement
- it reflects the company’s capability in integrating core sensors into medical devices
- it positions the company not only as a guidewire developer, but as a “device + sensing” developer
6. The four questions a good FFR article should answer
From a website-content standpoint, the most important questions are:
What does it measure
Not simply stenosis severity, but the functional impact of a lesion on coronary blood flow.
Why does it matter
Because anatomical narrowing and real ischemia are not always the same thing.
Why does it have gold-standard meaning
Because invasive wire-based FFR has long served as a key reference point in coronary physiology and in studies guiding revascularization strategy.
Why does the fiber-optic route deserve separate attention
Because it supports high-sensitivity pressure measurement while also expressing sensor-integration capability in miniature medical devices.
7. What this means for future website content
The FFR pressure guidewire is a strong anchor for ongoing content such as:
- FFR versus angiography
- why intermediate lesions need physiological assessment
- the role of coronary physiology in PCI decision-making
- why fiber-optic pressure sensing matters in miniature devices
This kind of content is useful not only for search visibility, but also for technical communication and partner education.
References
These references support website-level medical and technical interpretation. Final indications, product performance statements, and procedural claims should follow formal registration materials and IFU documentation.
- 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization.
https://www.acc.org/Guidelines/Guidelines/2021/12/09/18/18/Coronary-Artery-Revascularization - 2024 ESC Guidelines for the Management of Chronic Coronary Syndromes.
https://www.escardio.org/guidelines/clinical-practice-guidelines/all-esc-practice-guidelines/chronic-coronary-syndromes/ - Visual-Functional Mismatch Between Coronary Angiography, Fractional Flow Reserve, and Quantitative Coronary Angiography.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5114133/ - Coronary Angiography With Pressure Wire and Fractional Flow Reserve: State of the Art in the Diagnosis of Coronary Stenosis.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6514382/ - Optical Fibre Pressure Sensors in Medical Applications.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4541926/